





Plato was wrong. Millenia ago, as Ties Boerma—in his calm cadence and Dutch accent—tells a 2023 workshop of global public health experts, Plato said a good decision is based on knowledge, not numbers.
A Canada Research Chair of Population and Global Health at UM, Boerma is about as allergic to Plato’s sentiment as you can get.
For eight years he has directed Countdown2030, a global collaboration of universities generating evidence of what makes mothers and their children healthy in an effort to achieve the United Nations’ Sustainable Development Goals in low- and middle-income countries. Boerma, whose work is funded by the Bill & Melinda Gates Foundation, has amassed scores of numbers that enable us to make better decisions, saving more women and babies in countries where their risk of dying before a fifth birthday has declined impressively in the past two decades but is still as high as 31 in 1,000 live births (India) and 47 in 1,000 (Ethiopia). In Canada, it is 5 in 1,000.
In addition to asking why people are getting sick and dying in such countries, Boerma and the team focus on why they are not. Such “positive public health” can guide us in new ways and on Aug. 23, 2023, Boerma and his partners met in New Delhi to release the Gates-Foundation-funded Exemplars Report that confidently gives the global health community—and, perhaps most importantly, policymakers—numerical evidence on what drives progress.
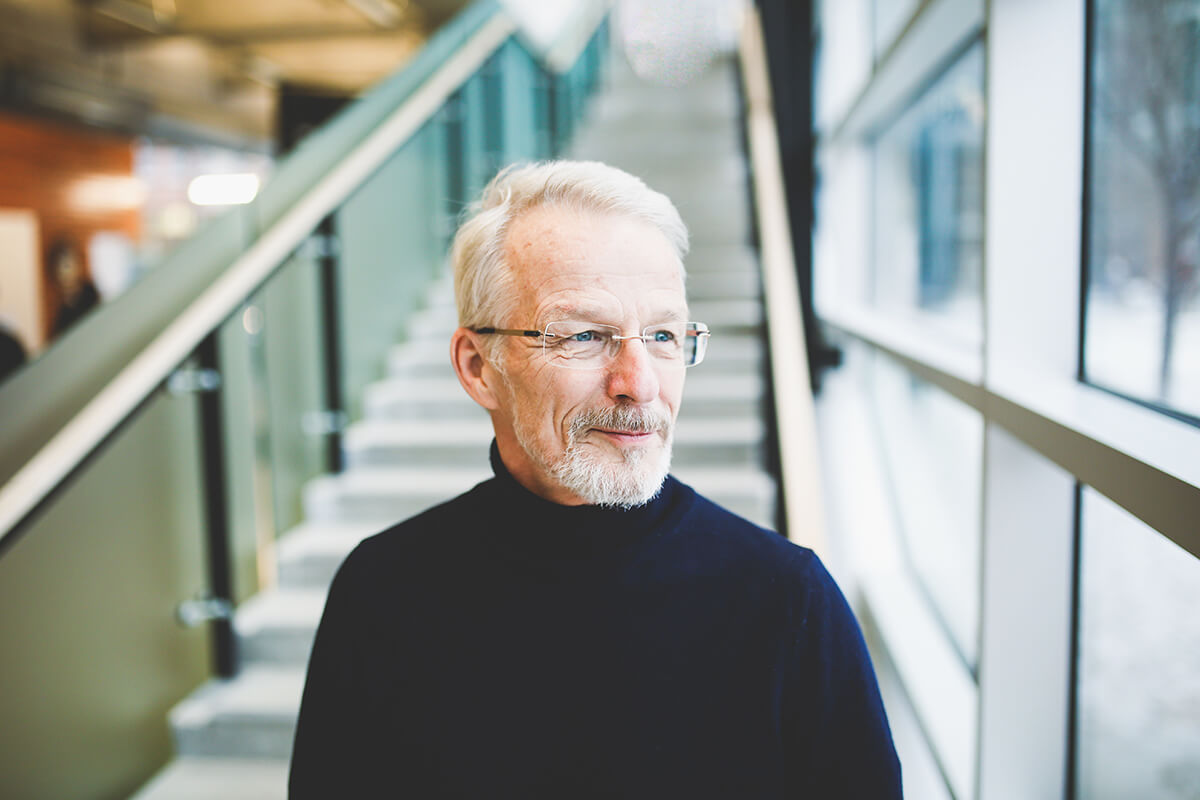
Ties Boerma on the Bannatyne campus // This photo and above by Rachael King
“It’s a difficult world right now,” Boerma says, “with climate change and conflict and the debt of crisis we see for poorer countries. There are many things that are really depressing. And you wonder, what progress can we make still? But we should also look at things that are going well and why they’re going well. I think it’s an important story and the experience we had in India is an important one and it can inform the way forward.”
Boerma’s talking about the focused efforts of UM’s Institute for Global Public Health (IGPH) in India, spanning more than two decades and led by epidemiologist Dr. James Blanchard [BSc(Med)/86, MD/86], which helped push the needle. In the last 20 years, the country has seen preventable deaths in children fall more than 70 per cent.
But how can the success there, with its unique politics, demographics, culture and geography be transferred to another distinct country? It’s a question that nagged Boerma from the outset of Countdown, running through his mind as he biked or swam, trying to decompress, which is why his team had to tackle it at their first meeting, and why they invented a new model called the “maternal, stillbirth and neonatal mortality transition model,” published in Lancet Global Health (PDF). Now adopted by the World Health Organization (WHO), it allows countries to track their progress by comparing their situation to data markers that guide the path upwards through five phases. Newborn deaths are high? Improve delivery care and invest in neonatal care units. Infant and toddler mortality is high in a poorer country? Strengthen immunization services and the treatment of pneumonia and diarrhea. And so on through increasingly complex social and health interventions.
It may sound basic but defining the big picture and distilling the solution into small, navigable—and universal—steps proved to be a massive undertaking and one the Rady Faculty of Health Science’s institute is uniquely equipped to help lead. IGHP has been instrumental in its long-term partnership with local governments and researchers, helping set up data tracking and scaling up initiatives and training that have meant fewer unnecessary deaths. In India, it has informed government efforts to build and distribute resources in targeted, life-changing ways.
What does it all matter if you publish findings no one uses? It’s more about collaborating with a country’s researchers and institutions.
In 2022, the Bill & Melinda Gates Foundation—a long-time champion of UM’s work in global public health—pledged another $20 million annually for five years, supporting partnerships in Uttar Pradesh to drive down maternal and neonatal mortality rates.
Boerma, a former director at WHO, joined UM seven years ago.
“I came to Manitoba and to the IGPH because of the philosophy of that team and of the department of community health sciences—to do science that is practical and embedded. To learn from real-life situations and try to come up with something that can be translated into practical tools for governments or civil society organizations.”
So he admits he was anxious when a key politician was late to the August launch of their research results in India, worrying they did not get government buy-in.
“What does it all matter if you publish findings no one uses? It’s more about collaborating with a country’s researchers and institutions”—in this case, the Mumbai Institute for Population Studies—”and whenever possible, bring the Ministry of Health in as well to get shared ownership over a study like this. I think that’s the most important part of it because our research, without jeopardizing its objectivity, needs to be embedded in decision-making systems.”

Josée Lavoie has spent her career working across the prairies and in the North // Photos by Katie Lenhart
Josée Lavoie, a professor of community health sciences at UM, invites you to imagine a real-world scenario.
You live in a remote Manitoban community and your kidneys are failing—they’ve likely been an issue since you were about 10 years old. There should have been interventions to prevent you from getting to this stage, but here you are laying in a hospital bed far from home as the sixth and final bag of today’s dialysis solution flows through a catheter towards your stomach.
All of this solution—a month’s worth weighs about a ton—has to be carefully stored. The clinic in your community doesn’t have space, and you ponder if the floors of your own house could even support this staggering weight. Your only option is to travel afar every week to lay there for three days before going home for a bit. What to do?
“If you have kidney disease in a First Nations community in Manitoba, many patients progress very quickly to dialysis and some prefer to die because dialysis is no way of living,” says Lavoie. “In this province we’re so urban-centric. It’s amazing to me what I can access in Winnipeg, but as soon as you leave the community that’s no longer accessible in a timely manner…. It’s a tremendous burden, but kidney disease can be arrested…with just simple follow-throughs on people found to have high blood pressure.”
This is how Ongomiizwin–Indigenous Institute of Health and Healing at UM helps. Its Anishnabemowin name captures the concept of “clearing a path for generations to come.” It is a unique university-community initiative in Canada because it aims to dismantle colonial structures while improving health outcomes. The predecessor of its health services wing goes back more than 50 years, to the launch of the J. A. Hildes Northern Medical Unit in 1970, the first to fly physicians and specialists to the North.

The scope of education and care offered today is vast—from increasing the number of Indigenous health practitioners to treating patients across Manitoba and Nunavut, to leading vaccination programs during COVID. There are also more than 60 researchers working in Manitoba and across Canada, as well as in Belize, Colombia, Australia, New Zealand and circumpolar countries, partnering with Indigenous groups to co-create solutions for better health.
For instance, community health science’s Javier Mignone has studied links between dangerous tick infestations and housing conditions in Colombia and today continues to work with local Indigenous organizations in assessing intercultural health initiatives, while colleague Andrew Hatala and his graduate students examine the barriers to care Belizeans living with Type 2 diabetes faced before and during the COVID-19 pandemic.
When compared to other Canadian universities, UM has the capacity to lead in initiatives like these because of long-established partnerships and trust grown and maintained over decades.
By working with a partner, I’m ensuring that they have the evidence and that they can quote the data and put it forward at the policy table so that they can move that system forward.
Now the outgoing director of Ongomiizwin Research, in the Rady Faculty of Health Sciences, Lavoie has spent her career working across the prairies and the North with many organizations and governments. For the past three years she has collaborated with the First Nations Health and Social Secretariat of Manitoba to address renal care discrepancies—looking at what care models bring the best outcomes.
Manitoba has the highest rates of kidney failure per capita than any other province. And renal disease is prevalent among rural and northern First Nations communities due to a multitude of reasons, but most notably, because there is a failure of primary care. Where, though, is the failure? Is there a barrier to access, or is the care not responsive, or is it that the tools being used are not appropriate or adapted to First Nations needs? This theme of questioning runs through many of Lavoie’s research projects.
The team identified 12,613 First Nations people with chronic kidney disease and found that those who lived in communities that only had a nursing station—which is the reality for most remote communities—fared the worst. But, if that station gets additional Indigenous programs, then follow-up care increases significantly.
“Our partner, the First Nations Health and Social Secretariat of Manitoba, lead the project because they know the communities. They have the capacity. They have the understanding…and we support them in their actions so that whatever is produced in the study is not a theoretical paper but an action plan. It’s transformative research, always.”
First Nations governments take the lead and ownership. For Lavoie and Ongomiizwin, this is vital.
“I engage with Indigenous governments because it doesn’t matter what I—a non-Indigenous researcher—say to the federal government. Unless a First Nation political organization takes it on and brings it to the policy table, it will not have traction because the federal government will listen to them, not to me. And that’s exactly what should happen. And so by working with a partner, I’m ensuring that they have the evidence and that they can quote the data and put it forward at the policy table so that they can move that system forward.”